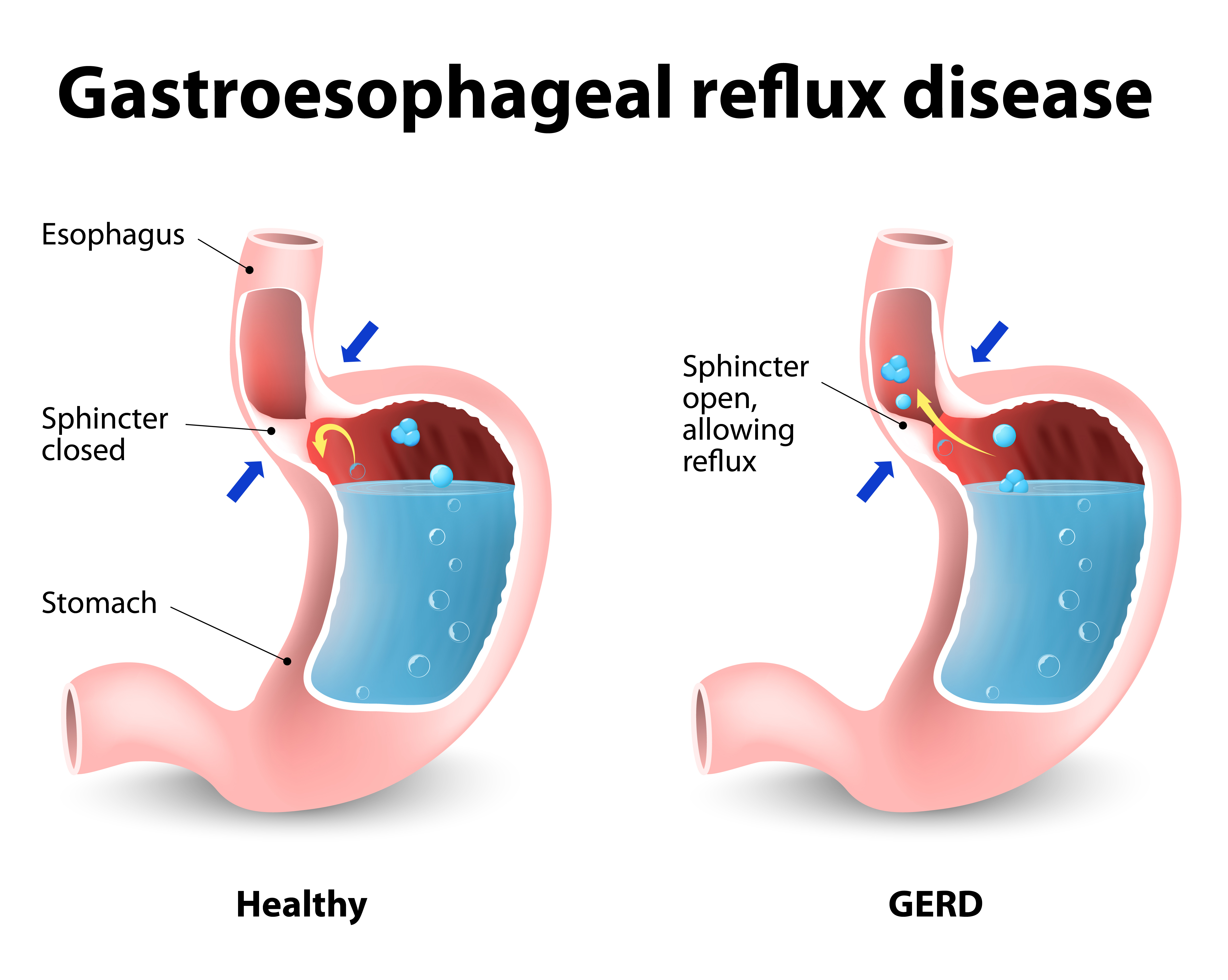
It is a condition where the liquid stomach acids leak backwards from the stomach into the esophagus. This results in the erosion of the esophagus- esophagitis and further potential lesions including stenosis, hemorrhage, ulcers, dysplasia, even carcinogenesis.
Causes:
Diaphragmatic hernia
Failure of the lower esophageal sphincter
Secondarily (following vomiting)
Pregnancy
Congenital
Systemic conditions (scleroderma, myopathies, burns, diseases of the central nervous system)
Symptoms:
Retrosternal pain (70%)
Regurgitation and aspiration (50%)
Dysphagia (40%)
Weight loss, anemia, loss of blood (0-10%)
Diagnosis:
- Endoscopy
- Oesophagography
- pH-test
- Oesophageal clearance test
- Manometry
Treatment:
- Conservative
Avoid the consumption of alcohol and smoking;
Small and frequent meals;
Pharmaceutical treatment (H2 inhibitors, proton pump inhibitors)
- Surgery
Anti-reflux surgery (Nissen, Hill, Blesey) in the absence of stricture;
In stricture: Dilatation, stricture plastic surgery, oesophagectomy.
Since 1990 onwards, the open surgery for GERD has been replaced by laparoscopic techniques with better results and virtually no chances of interoperative complications.
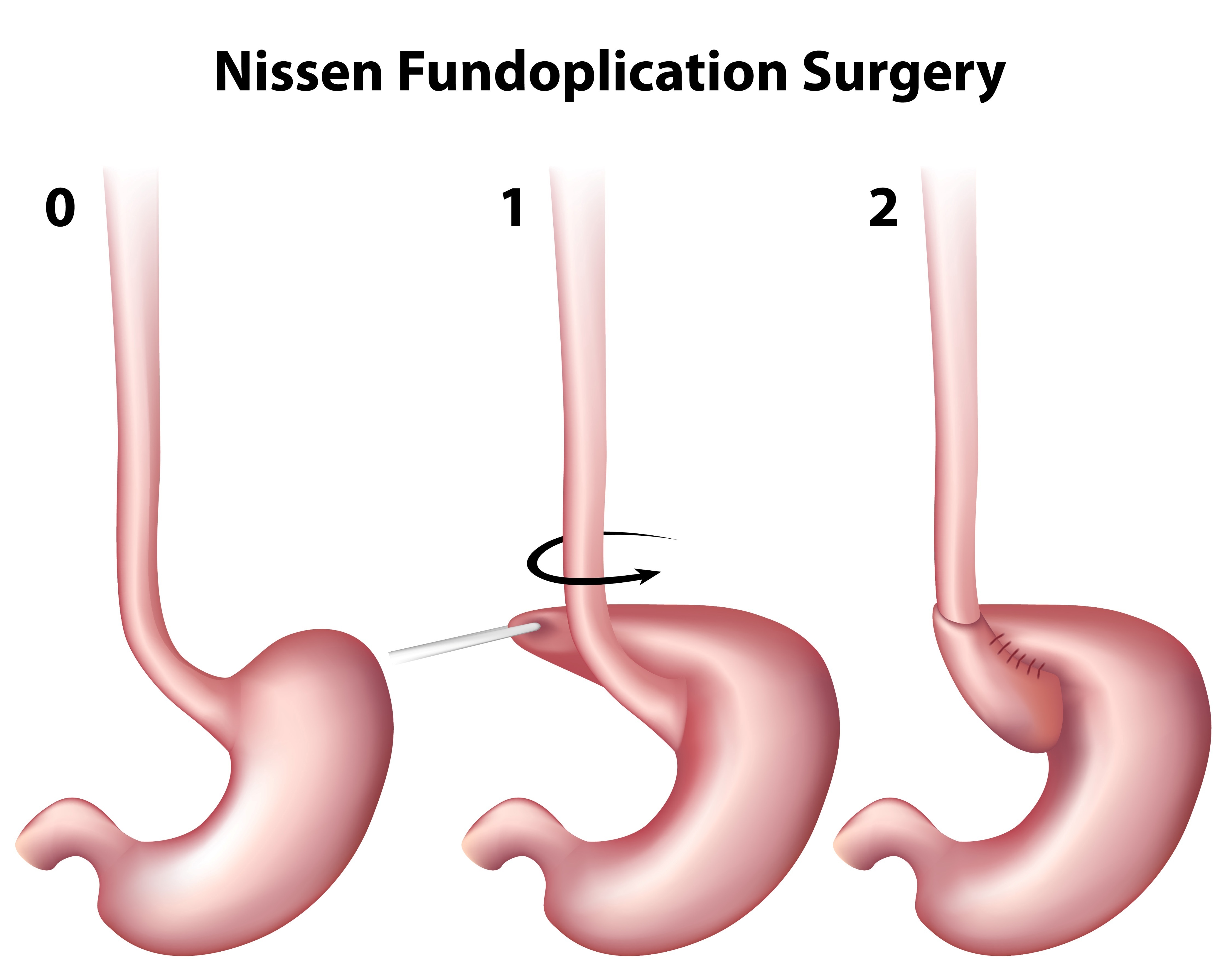
During the surgical treatment of GERD, we restore and correct the diaphragmatocele, we converge (“close” using sutures) the crura of the diaphragm and lower gastroesophageal sphincter by wrapping the fundus of the stomach around the lower part of the esophagus. Two techniques are used: Laparoscopic Nissen fundoplication or 360° wrap and, laparoscopic Toupet fundoplication or 270° wrap.
In the surgical treatment of GERD, we make 4-5 small incisions (5 mm each) on the skin without dissecting the muscles. The laparoscope, connected to a state-of-the art mini video camera enables the surgeon to monitor the patient’s internal organs by magnification of 10-15 times on a screen.
Laparoscopy outcomes
Studies have demonstrated that patients are completely free or show clear signs of improvement of GERD symptoms, immediately after surgery.
The great advantages of laparoscopy are the much lower postoperative pain, shorter hospitalization, very quick return to work, and spectacularly better esthetic results.
Posters created for all surgical conferences in the US and Europe prove that Laparoscopic Fundoplication is better in terms of long term results compared to conservative treatment and is associated with significantly lower morbidity and mortality vs open surgery. Also, its cost is lower compared to long term medical treatment.
Patients cease to use medication and improve their quality of life.
Are there any risks involved in anti-reflux surgery?
Complications are virtually non-existent if laparoscopic surgery is performed by a specialized surgical team with long-standing experience. Despite the above, as in all surgical processes, some complications may occur during anti-reflux surgery.