Peritoneum is a thin and transparent serous membrane lining the peritoneal and pelvic cavity and all the viscera contained therein (liver, spleen, intestine, uterus, ovaries. etc.).
This membrane consists of two layers: one lining the walls of the abdominal and pelvic cavities (parietal peritoneum) and the other that is investing and stabilizing the contained viscera (visceral peritoneum).
Peritoneal neoplasia, called “generalized peritoneal carcinomatosis” even today, is divided into the peritoneal carcinoma if the primary focus originates de novo from the epithelium and the peritoneal sarcomatosis if the primary lesion develops from mesenchymal cells. It is not a rare nosological entity because when an intrapelvic or intra-abdominal tumour is initially diagnosed it is already present in 10-15% of cases.
Peritoneal carcinomatosis involves tumors of advanced stages developing within the different intra-abdominal organs such as the intestine, the ovaries, the vermiform appendix, the stomach, the pancreas, and the liver. Furthermore, there are tumors developing directly from the peritoneum (mesothelium, pseudomyxoma). Luckily, this is an even less common type of tumor.
Peritoneal neoplasia could result from either spontaneous preoperative development or from iatrogenic intraoperative tumor dissemination. Tumor capsule rupture plays a critical part in the pathology and pathophysiology of tumor cell dissemination within the peritoneum.
The clinical prognostic factors for peritoneal malignancy include the malignancy extent and distribution, the presence/absence of remote metastases, the tumor grade, the implant size, and the adequacy of cytoreductive surgery, the extent of previous surgery, the age, the patient’s physical activity and the type of ascites occurred (hemorrhagic, serum or mucinous ascites).
Peritoneal cancer was considered as an inoperable pathologic entity that was not satisfactorily amenable to available chemotherapeutic agents. Currently, it is possible to surgically treat peritoneal cancer by combining cytoreductive surgery with treatment methods such as the Hyperthermic Intraperitoneal Chemotherapy (HIPEC).
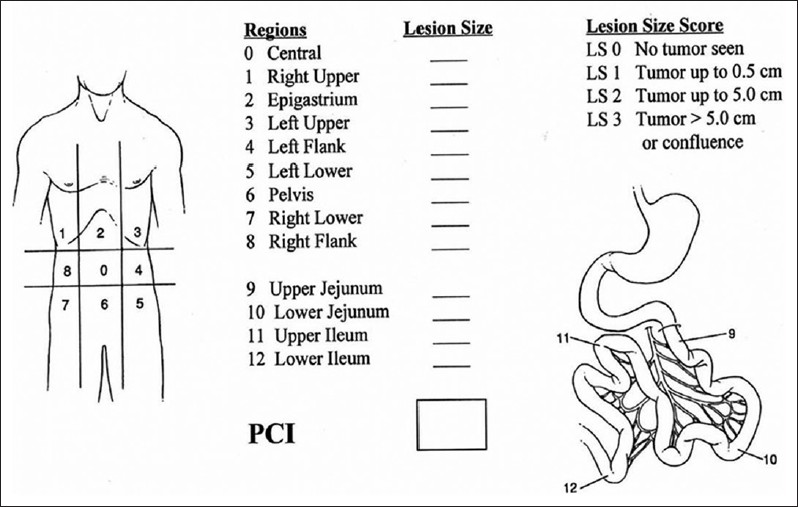
The extent of the peritoneal tumor is assessed using various methods and is one of the most important survival prognostic factors. The most detailed and accurate method for assessing it is the Peritoneal Cancer Index (PCI). This index is a simple figure which is the sum of the largest lesion from all 13 regions that form the abdomen, the pelvis, and the small intestine, according to this calculation method. The size of the largest lesions (lesion size or LS) is then calculated for each of the pelvic abdominal regions. In the absence of macroscopically visible tumor, the lesion is classified as LS-0. If the largest diameter of the lesion does not exceed 0.5cm, the lesion is then classified as LS-1, if it is >0.5cm and <5cm it is classified as LS-2 and if it is >5cm or if confluent lesions of various sizes are identified, it is classified as LS-3.
Peritoneal carcinomatosis Index is, therefore, the sum of the sizes of the largest lesions of each of the 13 regions pelvic abdominal regions (picture). PCI scoring is inversely associated to survival rates.
The advances of minimally invasive surgery have established it as a mainstream procedure for diagnosing and treating peritoneal neoplasia. Laparoscopic access presents many advantages including less postoperative pain, faster resumption of normal intestinal motility and shorter hospital stay.
Currently, peritoneal cancer staging is performed laparoscopically by surgeons adequately trained and experienced in laparoscopic and oncological surgery. Patients eligible for further surgical or non surgical treatment are evaluated and screened using diagnostic laparoscopy. Collaboration between experienced anatomic pathologists and oncologists results in a more effective treatment of the disease.